
Why the Quadriceps are Queen in ACL Rehab
Why?
Here are just a few of the reasons that quadriceps are queen 👑 in ACL rehab:
Rebuilding quadriceps muscle strength after ACL reconstruction correlates to better bone density in that tibia (and conversely, weaker quads correlate with decreases in bone density in the affected side's tibia).
Quadriceps weakness may have contributed to a ACL-injury in the first place.
Quadricep strength is key for decelerating the knee as an athlete pivots, cuts, jumps, or stops with speed.
Quad strength is associated with better outcomes, functional performance, return to sport, and decreased re-injury but research shows that quadriceps deficits still persist in approximately 30% of patients 12 months after surgery.
Quadriceps strength deficits prior to return to sport are a significant predictor of a knee re-injury. Every 1% increase in quadriceps strength correlates to a 3% reduction in re-injury rate.
Brief Anatomy:
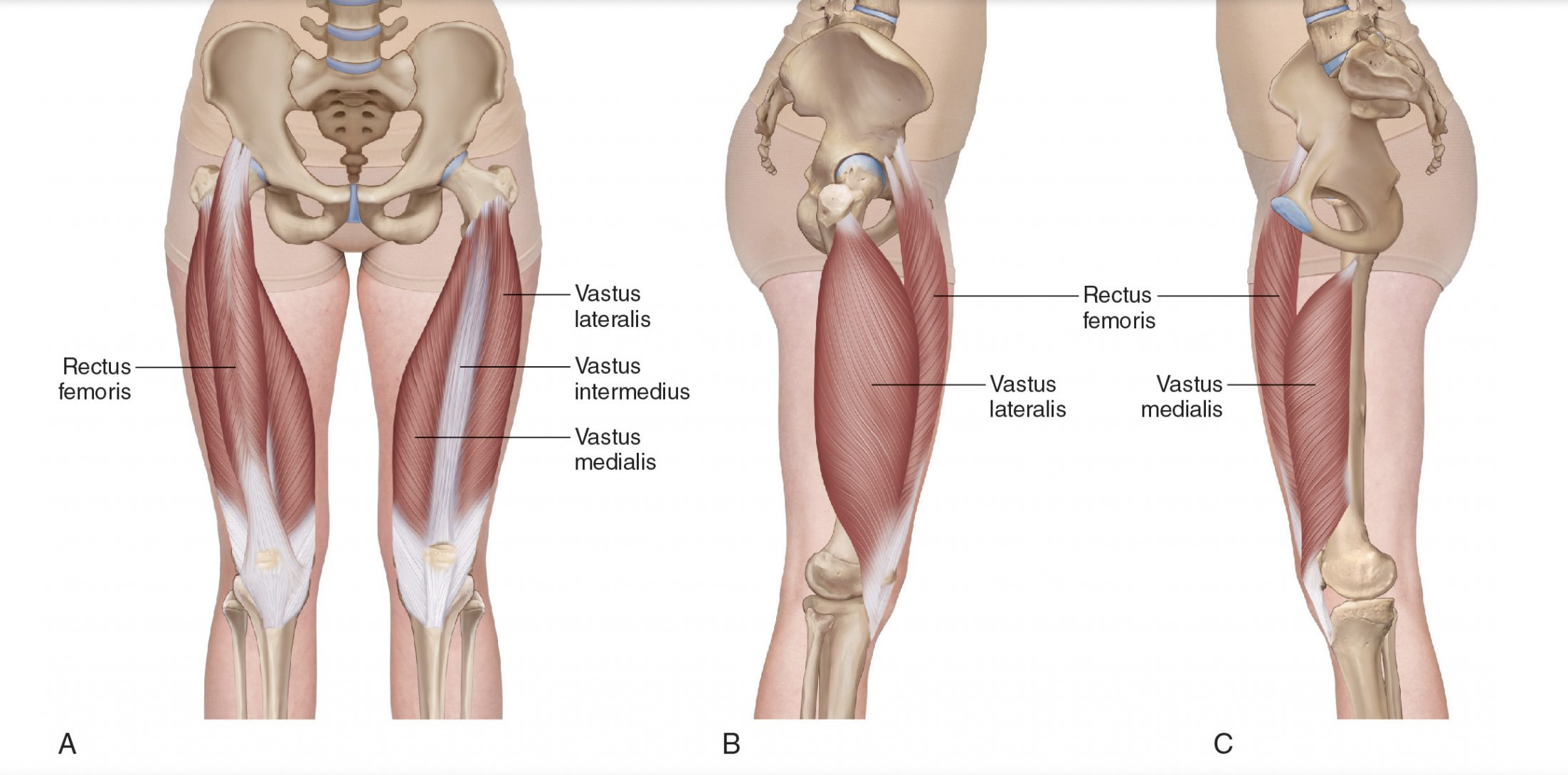
The quadriceps muscles are 4 distinct muscles:
the rectus femoris,
vastus lateralis,
vastus intermedius,
and vastus medialis
located in the front of the thigh. By the knee, they form a common tendon that contains the knee cap (patella) and attaches to the front of the tibia bone at a point called the tibial tuberosity.
The quadriceps muscles:
contract to straighten (or extend) the leg at the knee
and as the contraction slowly releases and the muscle lengthens (called an eccentric action) they work to control knee bending (flexion)
Quadriceps in ACL Rehab
The most important rehab check points after ACL injury and/or reconstruction involve the quadriceps muscles.
Initially:
One of our first goals is restoring quadriceps activation. After ACL injury and reconstruction, quadriceps weakness, activation failure, and atrophy (loss of muscle mass or size) quickly occur due to a complex phenomenon called arthrogenic muscle inhibition (AMI), in which an uninjured muscle becomes reflexively inhibited due injury of the joint it surrounds.
If you’re curious, here is a deeper explanation of the physiology:
Normally, an impulse travels along a motor neuron from the spinal cord to the muscle and causes a contraction when it reaches the muscle. With AMI, these impulses are inhibited, so the quadriceps muscle is capable of contracting, it just isn’t receiving signal from the spinal cord to contract.
I make sense of this by rationalizing that if one’s knee is injured, the body will want to keep them from running, jumping, etc. on that injured knee, so in order to protect itself, it decreases the amount of force they can create with the muscles around that joint, specifically the quadriceps.
Anyway, we can navigate this inhibition and help prevent loss of quadricep strength and size with a few strategies:
Using sensory stimulation via transcutaneous electrical nerve stimulation (TENS), joint cooling (cryotherapy), or vibration around the knee joint at the beginning of a rehab session to stimulate the nervous system (increasing the impulses traveling along nerves between the knee and the spinal cord) and create a ”therapeutic window” during which neural connections to the quadriceps muscles are increased and quadriceps-targeting exercises will be more effective.
Using Neuromuscular Electrical Stimulation (NMES, a modality similar to TENS but at a frequency that will cause a muscle contraction instead of just a sensory response) during quadriceps exercises to bypass the neural inhibition.
Using Blood Flow Restriction (BFR) during therapeutic exercise to maximize the benefits of low-load exercise.
Signs of progress here are a patient who gains the ability to fully weight bear on their affected limb, perform prolonged muscle contractions, and perform a set of straight leg raises while keeping the knee joint straight (or fully extended) without any sign of knee “lagging,” as well as increases in quadriceps strength output and size (measured by limb circumference). These efforts last from immediately post-op to around weeks 12-16.
Mid-Stage Rehab:
Our mid-stage rehab goal for the quadriceps is to increase strength so it is comparable to the quadriceps strength on the other/uninjured limb and so that it has the capacity to produce force relative to the individuals’s body weight. We start objectively testing quadriceps strength with a force transducer set up at about 12 weeks post-surgery.

The measurements we use here are called the Quadriceps Limb Symmetry Index (LSI) and Torque-to-Bodyweight Ratio (TTBW).
Limb Symmetry Index (LSI) is the comparison of the injured side’s strength as a percent of the uninjured side’s strength.
For example: if the uninjured side’s quadriceps produced 100kg of force and the injured side’s quadriceps produced 80kg of force, the LSI would be 80%.
In terms of Quadriceps LSI, we like to see above 70% before returning to linear running and 90% or greater (ideally, 95% or higher) by the end of the rehab journey.
The major limitation of this measure is: What if the opposite side’s quadriceps aren’t strong enough to begin with? Quadriceps strength (or lack of strength) on the uninjured side could have been a contributing factor to the initial injury or could have decreased while rehab efforts focused on addressing the injured side. Additionally, I’ve worked with many cases of ACL re-injury on the opposite limb where the LSI comparison becomes one of comparing the currently injured limb to the previously injured (and likely not fully rehabbed) limb.
This is why we also measure a ratio of quadriceps strength (torque) compared to the individual’s body weight. I like athletes to achieve around 2Nm/Kg torque to body weight ratio (TTBW) before initiating linear running (running in a line without changes of direction) and then, honestly, as high of a ratio as we can get after that.
The need for building serious quadriceps strength during ACL rehab is one of the reasons I believe it can be unethical for a PT clinic that doesn't have access to means of loading (i.e. barbells/dumbbells/KBs/leg extension machines) to work with athletes after ACL-reconstruction beyond the first 3ish months of rehab.
Late-Stage Rehab:
In late-stage rehab, our goal for the quadriceps is to restore the speed of contraction, called rate of force development. I often explain to patients that first we want to make sure their quadriceps have the capacity (via absolute strength) to decelerate their bodyweight when they want to cut or pivot, then we make sure that the quadriceps can activate in the split second those movement decisions occur on the field.
As a clinician, I’m still learning how to objectively measure this without taking out the equivalent to my current student loans to pay for the machines that do so accurately and reliably. For now, I subjectively look at quality of movement over many many reps of single leg landings (from various heights, directions, demands) and plyometric exercises.
Absolutes in ACL Rehab
So how do you know if the rehab professional you are working with is appropriately addressing your quads?
Easy: They are objectively testing quadriceps strength with a device that measures force output. They should use a a consistent set up, begin measuring around week 12, repeat measurements every 4-6 weeks after that, and be looking at this number in terms of limb symmetry and torque to body weight ratio.
And no, just measuring quadriceps strength with their hands is not enough.
Do I have to say it?
I do. Because this is the internet and someone’s going to come at me if I don’t.
OF COURSE we address other areas (hamstrings, glutes, calves, jumping, sprinting, landing, etc) in addition to our quad strengthening efforts.
We build robust strength and athletic capacity through the entire lower body during ACL rehab.
BUT if I had to say what our TOP priority is during rehab and where most rehab journeys fall short, it’s the quadriceps.
What Now?
Want to hear more about this and other rehab topics? Subscribe to my “Stay in the Game” email list.
Have a friend, teammate, or loved one going through rehab after an ACL injury? Share this blog post with them.
Interested in working together during your own recovery journey? Book a discovery call and let’s go measure your quad strength.